DermaFrac®: An Innovative New Treatment for Periorbital Melanosis in a Dark-Skinned Male Patient
Kanika Sahni and Martin Kassir1
Author information Copyright and License information Disclaimer
Abstract
Periorbital melanosis (under eye dark circles) is an often idiopathic cosmetically disturbing condition that is poorly responsive to currently available treatment modalities. We present the case of a 48-year-old man (skin phototype V) with significant idiopathic periorbital melanosis and who had good to excellent reduction in periorbital melanosis with the new DermaFrac®, which combines microneedling with simultaneous infusion of a serum containing active ingredients. The possible mechanisms of benefit are discussed. DermaFrac® may be an innovative and effective new treatment option for patients with periorbital melanosis.
INTRODUCTION
Periorbital melanosis (dark circles under the eye) is a frustrating condition with a multifactorial pathogenesis including genetic or constitutional pigmentation, dermal melanocytosis, post inflammatory hyperpigmentation secondary to atopic and allergic contact dermatitis, excessive subcutaneous vascularity, hormonal abnormalities, pigmentary demarcation lines, shadowing due to skin laxity, and tear trough associated with aging. When no cause is apparent, it is also termed idiopathic cutaneous hyperchromia of the orbital region (ICHOR).[1] It is commonly observed in dark-skinned patients, especially Asians, but there is only little data in scientific literature. A number of treatment modalities have been tried for this condition with mixed results, including topical agents,[2] chemical peels,[3] lasers like the Q-switched Nd: YAG laser[4] and even fat transplantation.[5] None of the treatments is uniformly effective and there is a need for newer approaches to its management.
CASE REPORT
A 48-year-old Indian male (skin type V) presented with complaints of dark circles under his eyes for past 2 years. It had started with light brown pigmentation under his eyes that gradually worsened to brownish black, velvety looking skin at the time of presentation. He was also bothered with the dryness, uneven texture and fine lines on the skin of his face. His past medical history was significant for hypothyroidism (currently euthyroid on oral levothyroxine 100 μg daily) and hyperlipidemia well controlled on rosuvastatin. There was no history of anaemia, diabetes, hypertension or any other significant medical or surgical illness. There was no personal or family history of atopy. He was not on any topical eye medications. His occupation involved working on the computer for 6-8 h a day.
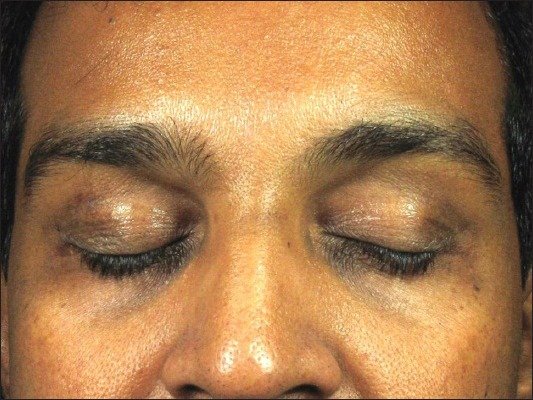
General physical examination was normal. In the infraorbital area, there was dark brown-black pigmentation extending along the tear trough onto the lower eyelid with thickened skin with a subtle velvety texture [Figure 1]. On stretching the skin, there were no congested vessels visible and there was no obvious scleral pigmentation. There was some hyperpigmentation of the upper eyelid also, which was more prominent laterally than medially. He did not have any significant pigmentation of the skin on his forehead, neck or cheeks, and there was no evidence of acanthosis nigricans elsewhere and no pigmentary demarcation lines on his perioral area or limbs. His haemoglobin was 14.2 and peripheral smear was normocytic normochromic.
Figure 1: Prominent brownish black hyperpigmentation with velvety texture of skin on upper and lower eyelids of a 48-year-old Indian male
We decided to treat him using the new DermaFrac® treatment that combines microchanneling using precisely calibrated needle penetration with simultaneous vacuum-assisted serum infusion. He underwent 12 DermaFrac® treatments (at 2 weekly intervals) for his entire face and forehead using the hand-piece with a 0.25-mm tip-cap at a pressure of 10 mmHg. After disinfection of the skin, two passes were given at each sitting. Anti-aging serum (containing meristoyl pentapeptide 17 sympeptide, acetyl octapeptide-3 SNAP 8, palmitoyl pentapeptide-4 matrixyl, acetyl hexapeptide-8 argirilene and tripeptide syn-ake) was infused for 10 sessions and the lightening serum (containing kojic acid) for 2 sessions. He was also advised to apply a tinted SPF 40 sunscreen in the morning all over his face. At each visit, the patient was asked to score the improvement on a visual analogue scale from 0 to 10, with 0 as no improvement and 10 as total clearance (Patient's Global Assessment, PGA).
The patient noticed gradually progressive improvement in his skin texture as well as marked improvement in his under eye dark circles [Figures [Figures22 and and3].3]. According to physician global assessment, there was 50–75% improvement in periorbital melanosis after 4 sittings and 75–90% improvement after 12 sittings, as assessed by 2 independent physicians. The patient reported improvement on a scale of 0 to 10, with 0 as no improvement and 10 as total clearance, with ‘5’ after four sittings and ‘7’ after twelve sittings. No side effects were observed, and the patient reported that he was comfortable and relaxed during the treatment sessions.
Figure 2: The study patient after 4 sittings of DermaFrac® procedures showing significant improvement in periorbital melanosis
Figure 3: The study patient after 12 sittings of DermaFrac® procedures showing sustained and further slower improvement in periorbital melanosis
DISCUSSION
DermaFrac® (Genesis Biosystems) uses a unique combination of technologies to enable improved topical infusion and dermal microinjury. It involves rolling a hand-piece with various tip caps on the skin, which pulls the skin under vacuum into contact with hundreds of micro-needles that penetrate the epidermis into the superficial papillary dermis while simultaneously introducing the infusion solution into the area [Figure 4]. The use of dermaroller or microneedling devices has previously been described for the effective management of scars,[6,7] skin laxity, wrinkles[8] and pigmented post-acne scars. The technique of microneedling, also known as percutaneous collagen induction, was pioneered by Fernandes, who initiated the use of a hand-held rolling cylindrical device mounted with numerous tiny needles.[9] Prior to that, the use of needles for the treatment of scars had been described by Orentreich et al., who reported successful use of the technique of subcision for acne scars.[10] This was followed by the use of a tattoo pistol for needle dermabrasion for the treatment of scars by Camirand and Doucet in 1997.[11] Microneedling relies on the principle of neocollagenesis and neovascularization developing due to the release of growth factors secondary to the piercing of the stratum corneum. These are believed to be responsible for the beneficial effects of the procedure in the treatment of scars and photo-aging.[9]
Figure 4: Schematic representation of hand-piece of DermaFrac® machine with microneedles penetrating the superficial dermis with vacuum-assisted simultaneous infusion
DermaFrac® is a newer modification of the microneedling technique that utilizes the microconduits created by the microneedling to simultaneously passively diffuse anti-aging peptides or other sera with pharmaceutical properties. Until date, there have been no reports with the use of this new technique for the treatment of under eye pigmentation. The possible mechanism of benefit in our patient was the improved hydration and the laying down of new collagen and elastin fibres in the skin, resulting in a thickening of the dermis that could possibly reduce the visibility of underlying congested vessels and any dermal pigment. The active components in the sera and their improved penetration into the skin secondary to microneedling may also have also contributed to the reduction in under eye dark circles.
This report illustrates the use of an innovative new, safe technique with virtually no downtime for the treatment of a frustrating cosmetically disturbing condition. Further larger studies are needed to confirm these initial encouraging results.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
1. Sarkar R. Idiopathic cutaneous hyperchromia at the orbital region or periorbital hyperpigmentation. J Cutan Aesthet Surg. 2012;5:183–4. [PMC free article] [PubMed] [Google Scholar]
2. Mitsuishi T, Shimoda T, Mitsui Y, Kuriyama Y, Kawana S. The effects of topical application of phytonadione, retinol and vitamins C and E on infraorbital dark circles and wrinkles of the lower eyelids. J Cosmet Dermatol. 2004;3:73–5. [PubMed] [Google Scholar]
3. Epstein JS. Management of infraorbital dark circles. A significant cosmetic concern. Arch Facial Plast Surg. 1999;1:303–7. [PubMed] [Google Scholar]
4. Ma G, Lin XX, Hu XJ, Jin YB, Chen H. Treatment of venous infraorbital dark circles using a long-pulsed 1,064-nm neodymium-doped yttrium aluminum garnet laser. Dermatol Surg. 2012;38:1277–82. [PubMed] [Google Scholar]
5. Roh MR, Kim TK, Chung KY. Treatment of infraorbital dark circles by autologous fat transplantation: A pilot study. Br J Dermatol. 2009;160:1022–5. [PubMed] [Google Scholar]
6. Doddaballapur S. Microneedling with dermaroller. J Cutan Aesthet Surg. 2009;2:110–1. [PMC free article] [PubMed] [Google Scholar]
7. Majid I. Microneedling therapy in atrophic facial scars: An objective assessment. J Cutan Aesthet Surg. 2009;2:26–30. [PMC free article] [PubMed] [Google Scholar]
8. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles and skin laxity. Plast Reconstr Surg. 2008;121:1421–9. [PubMed] [Google Scholar]
9. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17:51–63. [PubMed] [Google Scholar]
10. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21:543–9. [PubMed] [Google Scholar]
11. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997;21:48–51. [PubMed] [Google Scholar]
Articles from Journal of Cutaneous and Aesthetic Surgery are provided here courtesy of Wolters Kluwer -- Medknow Publications